

New French Distribution Agreement with Larylab® Technologie EIRL
September 11, 2020Minimally Invasive Stretta Antireflux Procedure Accessible to Millions more Patients
November 19, 2020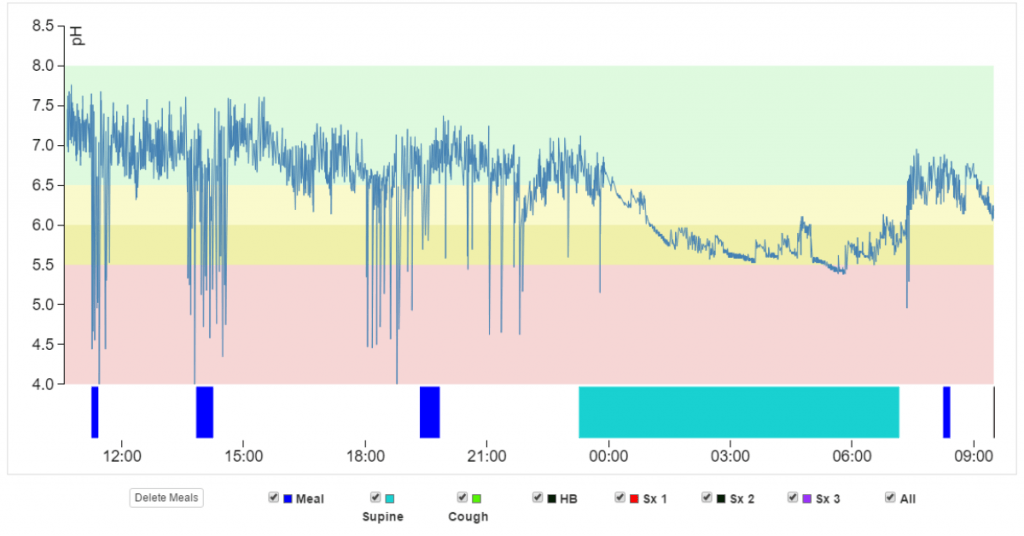
The Restech Dx-pH System as a valuable tool for surgical decision-making
By: Müller DT, MD; Leers JM, MD; Bruns CJ, MD; Fuchs HF, MD
Department of General, Visceral, Cancer and Transplant Surgery, University of Cologne
CASE HISTORY
53-year old male with a BMI of 24 kg/m2 presented with typical GERD symptoms such as severe bothersome heartburn every day, frequent belching, regurgitation especially after eating heavy meals, and occasional chest pain.
In addition, he reported atypical symptoms, mainly a chronic cough. His symptoms generally worsened after eating heavy meals, deep-fried foods, and alcohol consumption.
The patient presented at our Department of General, Visceral, Cancer and Transplant Surgery for further evaluation of his symptoms. Prior treatment included PPIs, however, sufficient symptom control was not achieved, and the patient sought alternative treatment options including surgery.
EVALUATION
The patient was seen in our specialized surgical outpatient clinic. Prior to receiving a complete diagnostic work-up, the patient discontinued PPIs for 7 days. Upper GI endoscopy revealed mild LA Grade A esophagitis and a 2 cm Hiatal Hernia. Biopsies of the gastroesophageal junction were taken, and the pathology report confirmed reflux-associated esophagitis.
To determine the exact position of the lower esophageal sphincter (LES) and as part of our preoperative evaluation, we proceeded with high-resolution manometry. This demonstrated 100% peristaltic swallows, an LES resting pressure well within the normal range, and an overall good esophageal motility.
Contrast radiography (barium swallow) was performed in both upright and supine positions and using Valsalva’s maneuver and did not confirm any abnormal reflux.
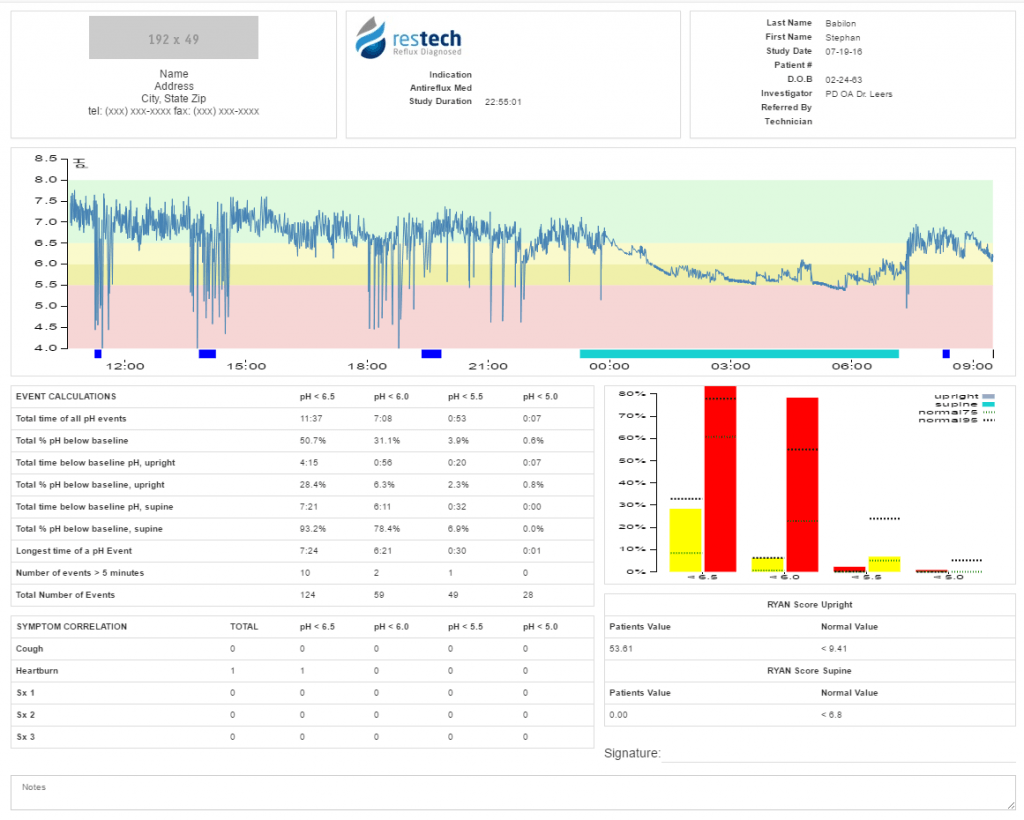
In order to further evaluate abnormal esophageal and/or laryngopharyngeal acid exposure we then performed simultaneous 24-hour impedance pH-metry and laryngopharyngeal pH-metry using the Restech Dx-pH. The esophageal pH probe was placed 5 cm above the LES as previously determined by high-resolution manometry. A total of 56 reflux episodes were recorded, though the patient was only below a pH of 4 for 2.1% of the study.
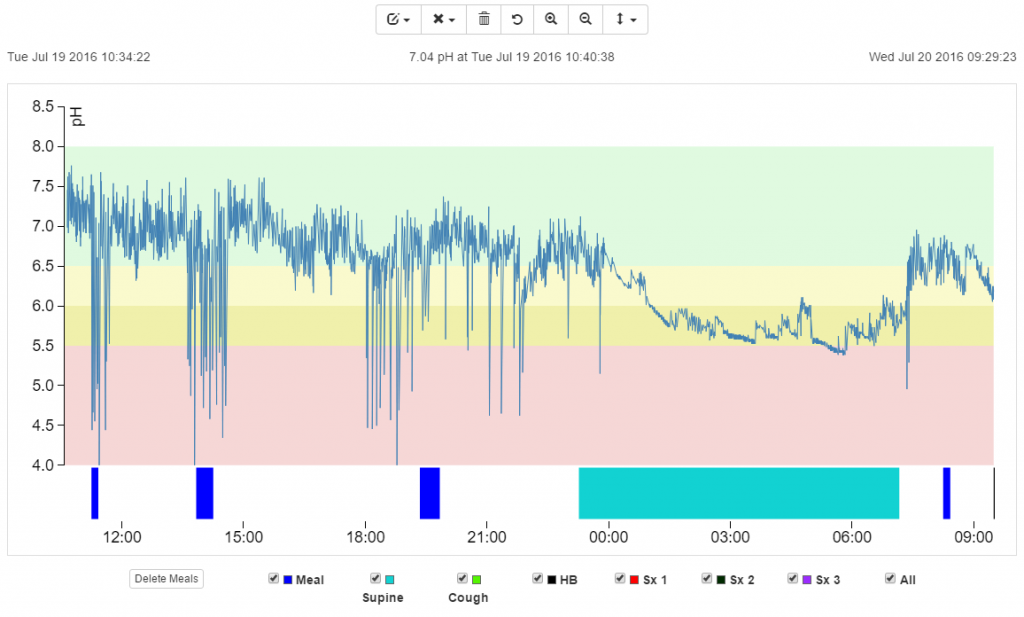
Our patient showed a borderline abnormal composite DeMeester score of 10.4 with the threshold for abnormal being > 14.72. This result alone does not clearly prove abnormal esophageal acid exposure.
In contrast, results from the concurrently performed Restech Dx-pH measurement showed clearly abnormal laryngopharyngeal acid exposure. An upright RYAN score of 52.13 was calculated using DataView 4, which exceeds the previously established normal threshold of 9.41, (Ayazi et al.,2009). Supine position showed a normal RYAN score of 0.
DIAGNOSIS
Given the mainly typical GERD symptoms and chronic cough, the endoscopic proof of reflux-related esophagitis, the borderline abnormal esophageal pH measurement, and the abnormal upright RYAN score on the Restech Dx-pH, a diagnosis of GERD with associated atypical symptoms was made. Due to the good esophageal motility and the previous failure of long-term PPI therapy, our patient was considered a good candidate for minimally invasive antireflux surgery.
TREATMENT
One month after the diagnostic evaluation, the patient underwent a laparoscopic Nissen fundoplication (360° fundoplication).
OUTCOME
At his one-year postoperative follow-up, the patient reported no use of any PPIs or anti-acid medication and the GERD-HRQL, used for assessment of symptoms, showed a score of 2. The patient reported full symptom resolution, with no heartburn or cough and only mild dysphagia. In addition, the patient stated that he was very satisfied, his overall health had improved, and if he had to choose a treatment again, he would once more opt for surgery.
CONCLUSION
As shown in earlier research, Restech’s Dx-pH test and 24-hour esophageal pH tests do not necessarily need to correspond. With a borderline DeMeester score, a positive Restech examination helped to support the decision for antireflux surgery, in this case leading to full symptom resolution for our patient.
KEY TAKEAWAYS
- Due to their multifactorial origin, atypical symptoms can be a great diagnostic challenge, as GERD can be either a cause or an aggravating cofactor.
- The Restech Dx-pH test and conventional esophageal pH tests do not necessarily need to correspond, as a variety of different reflux scenarios exist.
- In patients with a borderline abnormal esophageal pH measurement, the Restech Dx-pH test results can help support the decision for or against laparoscopic antireflux surgery.