
Stretta Presentations and New Data at DDW 2017 Highlight Positive Outcomes
May 30, 2017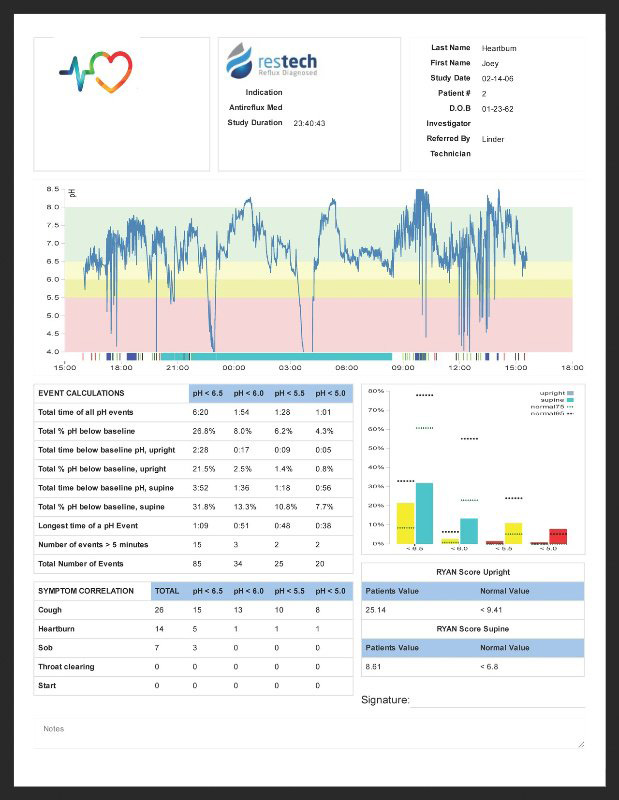
Restech’s NEW pH software!
August 1, 2017
1. SYMPTOMS DON’T TELL THE FULL STORY.
Empiric treatment with medication has long been the standard diagnostic tool for extraesophageal reflux. Presently, this approach is being challenged by new studies that suggest potential damage resulting from anti-reflux drugs. It is further complicated by a placebo effect mitigating symptoms while damaging acid persists. Given the multifactorial nature of laryngopharyngeal reflux, symptoms are not a reliable indication of how well reflux is being controlled.
%202F%20OropH%20Values%20IMAGE.jpg)
The charts above (adapted from Beaver, 2012) illustrate the similarities in presenting symptoms among patients with positive and negative pH studies.
2. OBTAIN A FASTER, MORE RELIABLE DIAGNOSIS.
In 24 hours or less, you can have an evidence-based diagnosis without exposing your patient to a 6-8 week empiric trial, only to arrive at a presumptive diagnosis based on symptom changes.
- Negative cases avoid PPI exposure and potential rebound acid hypersecretion
- Positive cases can be more precisely treated from the beginning vs. partial acid control camouflaged by placebo effect and symptom relief, while damaging exposure persists
3. RECORD A BASELINE.
Having a baseline of your patient’s “starting point” on file allows you to determine the efficacy of treatment and explore alternative treatments if needed.
PRE-TREATMENT pH STUDY RESULTS:

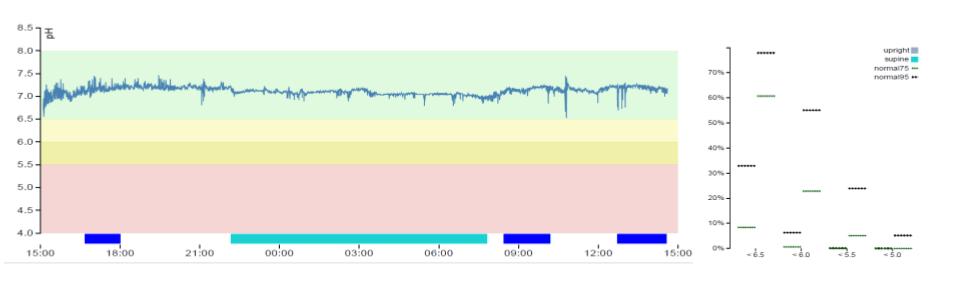
POST-TREATMENT IMPROVEMENT:

POST-TREATMENT RESOLUTION:
4. DESIGN A TARGETED TREATMENT PLAN.
Test results support developing a targeted treatment plan, customized for each particular patient’s needs.
- Titrate medications based on timing and severity of reflux episodes
- Avoid unnecessary medication
- Encourage lifestyle modifications for mild or marginal cases
- Triage for more aggressive treatment for the most severe cases
5. ACHIEVE BETTER PATIENT COMPLIANCE.
Studies demonstrate evidence-based treatment results in significantly better patient compliance. Patients tend to comply with the prescribed treatment plan when an objective pH study is performed prior to treatment.
| Method of Diagnosis | Compliance with medical therapy (p=.019) |
Compliance with lifestyle modifications (p=.0001) |
Reduction in RSI (p=.023) | |
| Group 1 (n=73) | pH monitoring | 68.5% | 82.2% | 36.6% |
| Group 2 (n=70) | Empiric treatment with PPIs | 50% | 25.7% | 24.4% |
References:
Beaver ME, Karow CM. Clinical Utility of 24 Hour Pharyngeal pH Monitoring for Hoarseness. J Laryngol Voice. 2012;2(2):60-3.
Friedman M, Maley A, Kelley K, et al. Impact of pH Monitoring on Laryngopharyngeal Reflux Treatment: Improved Compliance and Symptom Resolution. Otolaryngol Head Neck Surg.2011 ;144(4):558-62