
Stretta: A valuable endoscopic treatment modality for gastroesophageal reflux disease.
January 19, 2018
66 Year Old Male with Chronic Cough on Long-term PPIs
February 15, 2018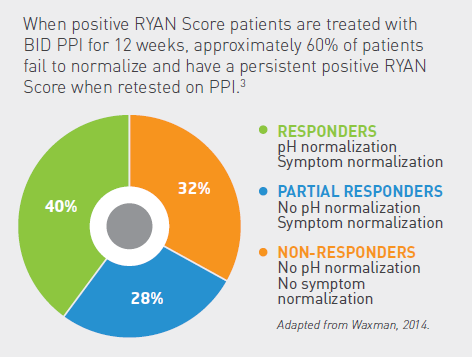
Heartburn and regurgitation are easily identifiable symptoms of gastroesophageal reflux disease (GERD) and tend to be easier to treat with PPI therapy. However, symptoms of laryngopharyngeal reflux (LPR) or atypical reflux have become very prevalent in the population since they are difficult to spot and are often unresponsive to PPI therapy.
Here are FOUR possible reasons why your patient’s LPR symptoms aren’t improving:
1. Their symptoms aren’t caused by reflux.
Common chronic conditions like cough, throat clearing, and laryngeal erythema are examples of LPR symptoms. However, these symptoms can also result from several other etiologies.1
- Acute Laryngitis
- Upper Respiratory Tract Infection (viral)
- Overuse of Voice (singing, talking, and/or shouting)
- Allergies
- Inhaling Environmental Irritants
- Smoking
- Neurological Conditions
2. Empiric treatment is ineffective at confirming LPR.
The absence of specific LPR symptoms and treatment methods make LPR a difficult condition to assess. Acid can cause LPR symptoms even in the absence of GERD. Although PPIs are extremely effective in controlling symptoms of GERD, PPI therapy has proven unreliable in managing LPR symptoms and confirming reflux as the etiology of patient complaints.
A systematic review of six randomized, controlled studies reveals that the majority of LPR symptoms improved similarly in the PPI and control groups.2 This data demonstrates that empiric PPI treatment of suspected LPR is not superior to treatment by placebo.
3. Laryngopharyngeal pH fails to normalize for most individuals following PPI therapy.
A study led by Jonathan Waxman, MD at the University of Illinois at Chicago, tested patients pre- and post-treatment after at least 4 weeks of PPI therapy. Only 39.5% of patients with positive RYAN Scores achieved both pH and symptom normalization while on PPIs. The remaining 60.5% of patients had persistent positive RYAN Scores with no pH normalization when retested on medication.3 (The RYAN Score was created by Dr. Tom DeMeester with high specificity for severe reflux patients using thresholds of pH 5.5 for upright and pH 5.0 for supine positions.)
Over 30% of patients presenting with LPR symptoms do not have excessive acid exposure; thus, LPR symptoms won’t improve in over 30% of patients on PPI therapy.3
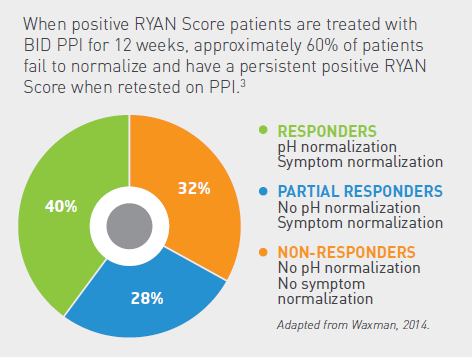
4. Symptom normalization does not equate to pH normalization.
Only significant improvement (not normalization) of the upright RYAN Score was necessary for symptom normalization. This further illustrates why symptoms are unreliable in the diagnosis of LPR. Acid exposure in the larynx in the absence of symptoms may lead to detrimental damage in sensitive epithelial tissue.
The chart above illustrates that symptom normalization while on PPIs does not correlate with a healthy patient. Testing on therapy at 8-12 weeks will either confirm pH normalization or identify patients who require escalated therapy or surgical intervention.
Visit our Restech blog to learn more about evidence-based pharyngeal pH testing.
… AND … download a copy of “Atypical Reflux: An Ever-Present Enigma in the Physician’s Office” for a concise overview of the current literature on laryngopharyngeal reflux, PPI response, and objective testing.
{{cta(‘fbbd62f5-eff1-479a-8b58-d256ed8d0b13’)}}
References
- Hoarseness. American Academy of Otolaryngology-Head and Neck Surgery. http://www.entnet.org/content/hoarseness. Published April 22, 2014.
- Karkos PD, Wilson JA. Empiric Treatment of Laryngopharyngeal Reflux with Proton Pump Inhibitors: A Systematic Review. Laryngoscope. 2006;116(1):144-8.
- Waxman J, Yalamanchali S, Valle ES, Pott T, Friedman M. Effects of Proton Pump Inhibitor Therapy for Laryngopharyngeal Reflux on Posttreatment Symptoms and Hypopharyngeal pH. Otolaryngol Head Neck Surg. 2014;150(6):1010-1017.